Achieve Better Visual Outcomes After Refractive Cataract Surgery
Achieve Better Visual Outcomes After Refractive Cataract Surgery
Did you know that cataracts are the leading cause of blindness in the world? There are more than 25 million Americans estimated to have cataracts, clouding of the eye’s lens, causing blurry vision.
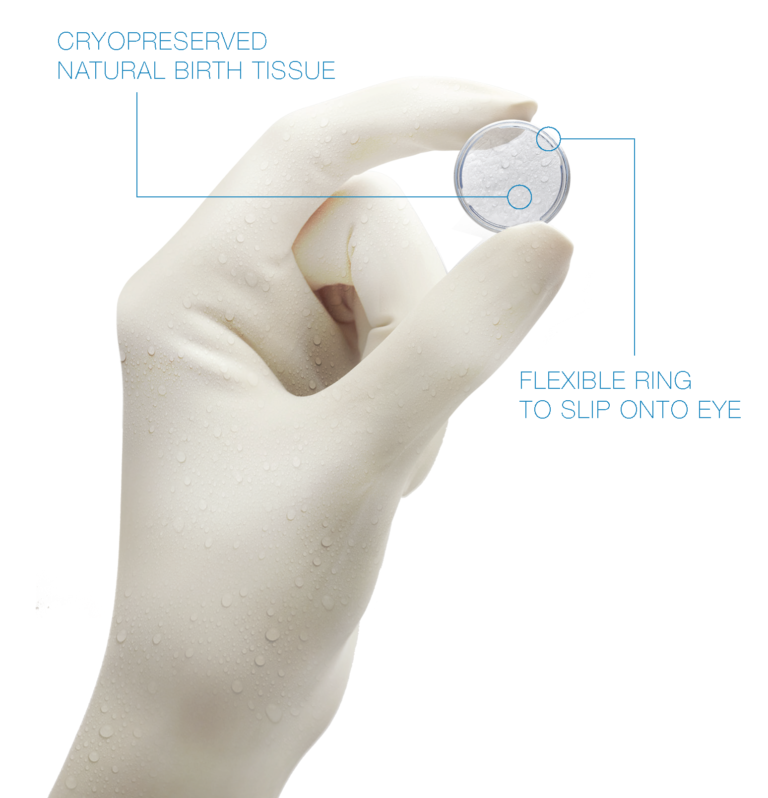
To ensure the opportunity for the best outcome for your patients, use PROKERA® for pre-cataract optimization.
In the recent annual American Society of Cataract and Refractive Surgery (ASCRS) Clinical Survey, it was noted that Ocular Surface Disease (OSD), including Dry-Eye Disease (DED), can affect the visual quality of patients undergoing keratorefractive and phacorefractive surgery significantly.8

In a survey done by the ASCRS in 2017, 83% of people indicated an algorithm for ocular surface diagnostics would be valuable due to lack of awareness of the most current OSD tools and guidelines.
THE IMPORTANCE OF OCULAR SURFACE OPTIMIZATION
THE IMPORTANCE OF OCULAR SURFACE OPTIMIZATION
Consequences of not treating Ocular Surface Diseases prior to Refractive Surgeries:

Intracular Lens (IOL) Calculation Errors
Preoperative lens measurements can be inaccurate, causing surgeons to implant the wrong type of lens, select the wrong lens power, misalign a toric lens, or even place astigmatism incisions at the wrong location.

Unsatisfactory Post-Surgical Visual Outcomes
A patient with a moderate to severe Ocular Surface Disease Index (OSDI) score can develop new visual symptoms in the postoperative period, which results in discomfort and overall dissatisfaction with the surgery.

New or Persistent OSD Signs & Symptoms
The ASCRS created a category of visually significant OSD with potentially adverse effects on visual quality and Snellen acuity, both pre & post-refractive cataract surgery. This new category determines whether the identified OSD sub-types will lead to refractive errors.

Reduced Retinal Image Quality
Tear film irregularities can reduce retinal image quality by 20% to 40% resulting in a residual reduction of retinal image quality after the cataract procedure.3

By treating OSD preoperatively, postoperative visual outcomes and patient satisfaction can be significantly improved. Furthermore, a greater proportion of patients report being “very satisfied” with their vision when there are no refractive errors.4
EVALUATION RESOURCES FOR OCULAR SURFACE OPTIMIZATION
EVALUATION RESOURCES FOR OCULAR SURFACE OPTIMIZATION
The ASCRS Cornea Clinical Committee defines Visually Significant Ocular Surface Disease in the cataract population as8:
Any combination of:
- Fluctuating vision that improves with blinking or lubrication
- Highly elevated osmolarity and MMP-9
- Irregular irregular fluctuating topography and/or aberrometry
- Interblink increases in OSI
- Irregular irregular astigmatism from corneal epithelial abnormatilies
- Significant corneal staining
NON-VISUALLY SIGNIFICANT OSD (NVS-OSD)
e.g., Normal cornea, normal topography (regular astigmatism, no corneal stain, stable vision)
- Does not impact preoperative measurements or post-surgical refractive outcomes
- Surgery proceeds
- Prophylactic treatment and patient education
VISUALLY SIGNIFICANT OSD (VS-OSD)
e.g., corneal abnormality, central PEE, irregular irregular astigmatism, abnormal osmolarity, fluctuating vision, etc.
- Can impact preoperative measurements and post-surgical outcomes
- Surgery must be delayed & biometry rechecked
- Requires intensive, rapid OSD treatment until condition is fully resolved
RMS Value
RMS Value can be an essential tool to quantify irregular & regular astigmatism.
0.3+ RMS indicates some degree of OSD.
0.4+ RMS indicates significant OSD usually involving a basement membrane dystrophy.
Identify asymptomatic patients who have nerve dysfunction by utilizing:
- Patient questionnaire/patient reported symptoms
- Abnormal test results (VS-OSD)
BENEFITS OF USING PROKERA FOR OCULAR SURFACE OPTIMIZATION
BENEFITS OF USING PROKERA FOR OCULAR SURFACE OPTIMIZATION

By consensus of the ASCRS Cornea Clinical Committee, the treatment of OSD, especially VS-OSD, in the preoperative patient population generally requires a more aggressive, often multifaceted approach with a targeted combination of prescription medications and procedural interventions to rapidly reverse OSD and minimize surgical delays.8
SUPERFICIAL OSD
Place PROKERA for 5 +/- 2 days, repeat biometry, schedule for surgery the same day after PROKERA removal.
BASEMENT MEMBRANE DYSTROPHIES
Superficial Keratectomy, allow cornea to normalize (about a month), repeat biometry, schedule surgery.
The ability of PROKERA to help normalize the ocular surface quickly in chronic dry eye patients and accelerate re-epithelialization after superficial keratectomy, or when there is evidence of limbal stem cell deficiency, makes it an essential part of the pre-cataract surgical regimen.5-7
Additionally, the ASCRS specifically highlighted the DREAM & Thomas John Nerve Regeneration Study to illustrate the ability of PROKERA to treat moderate & severe dry eye patients.8
